to 2020 (Blue). Click each image to enlarge")



|
|
Blog Feeds
The SakerA bird's eye view of the vineyard
Public InquiryInterested in maladministration. Estd. 2005
Lockdown Skeptics
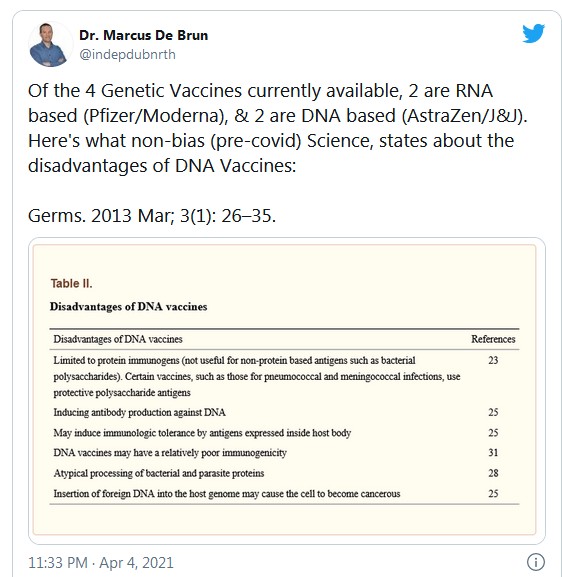
| Healthy People Do Not Require Genetic Vaccination international | health / disability issues | opinion/analysis international | health / disability issues | opinion/analysis  Friday April 09, 2021 22:13 Friday April 09, 2021 22:13 by Dr. Marcus De Brun by Dr. Marcus De Brun Having recently stated publicly that I would not administer a genetic-vaccine to a healthy animal, never mind a healthy human being, I have been asked by friends (and foes) to clarify this statement, and will attempt to do so here. Related Links: Doctors for Covid Ethics Demand Immediate Suspension of Gene Based Vaccines | Interview of Dr Mike Yeadon Dr Mike Yeadon, former CSO and VP, Allergy and Respiratory Research Head with Pfizer Global R&D and co-Founder of Ziarco Pharma Ltd, talks about his grave concerns about the Coronavirus jab Presently vaccines produced by four companies (Pfizer, Moderna, Astra Zeneca and Johnson & Johnson) are available on the European market. All four are genetic vaccines in that they are composed of synthetic DNA or RNA that is contained within a membrane or shell. In construction and appearance the vaccine is very similar to the SARS-CoV-2 virus responsible for the coronavirus disease known as Covid-19. The vaccine gains entry to human cells by a process that is almost identical to the manner by which a virus generally gains access to host cells. This process is called transfection. Each of these vaccines work by introducing either DNA or RNA into host cells. The genetic material then instructs host cells to make a piece of the coronavirus (the spike protein) that is then released into the blood stream or tissues. There, the spike protein will trigger an immune response. Following this immune response, the vaccinated individual will retain some immunity; they will have antibodies and white cells that can now recognise Covid-19 and attack it before it has a chance to cause a serious infection. The AstraZeneca and Johnson & Johnson vaccines are DNA vaccines,[i] which transfect DNA into the Nucleus of host cells. The Pfizer and Moderna Vaccines are RNA vaccines, these transfect their RNA into the cytoplasm of host cells. The difference will be explained later; however, the initial process is the same: human cells take up synthetic viral genes, those genes then direct those cells to begin manufacturing the spike-protein of Covid-19. The cells will then release the nascent spike-protein into the bloodstream or tissues, where it will then function as a traditional vaccine. In essence, the distinction between genetic-vaccines and traditional vaccines is that the latter would involve a person being injected with killed or inactive virus or spike-protein, which would then cause our immune systems to mount a response. Each of these novel genetic-vaccines however, insert genetic material into human cells. These synthetic genes then hijack those cells or convert them to manufacture and release the spike-protein. With a genetic vaccine, pharma does not make the vaccine, our own cells are programmed to do the work instead, a process entirely different from that of a traditional vaccine. Out with the OldFor the first time in my medical career of some twenty years, I am presented with the apparent necessity of vaccinating young healthy people with experimental vaccines, against a disease for which they have little or no risk of suffering life-threatening,[ii] or even serious long-term[iii] illness. The vast majority of vulnerable people, to whom they might pass Covid-19 to, have already been either vaccinated or been exposed to the virus.[iv] In Ireland according to our Central Statistics Office, during the past 12 months up to the end of January 2021; amongst the entire population of 1-24yr olds, there have been 55,565 PCR confirmed cases of Covid-19. Out of those cases, there has not been a single death recorded; from, by, or associated with Covid-19.[v] It has been reported that a single Covid-related death in this cohort (1-24yrs) did occur in February of this year. However, this has yet to appear in the figures published by the CSO. Young nurses, medical staff, care workers, are being pressured into taking a vaccine they probably dont need themselves, despite residents under their care having been almost all vaccinated already. Now Covid-19 genetic-vaccines are being tested upon children as young as six months old.[vi] A Scarcity of Serious Questions? Or a Scarcity of Serious Media?The justification for many, if not most, policies during this crisis has largely been based on mortality data. In contrast, Swedish authorities have enforced relatively few restrictions, nor made masks mandatory. In Ireland, the CSO indicate that 92% of all Covid-related deaths have occurred in those over 65 years of age.[vii] In Sweden that cohort of their population is 3.17 times greater Irelands. Thus, if we roughly compare the Swedish mortality total (at the time of writing) of 13,262, to the Irish total of 4588, and if we then multiply the Irish mortality total by 3.17, we arrive at a figure of 14,544, which is significantly higher than the comparable Swedish total. We are crudely, but reasonably, comparing like with like to reveal glaring potential problems with our own relatively draconian Covid policies. When compared with Sweden, our own version of lockdown seems to have had no benefit in terms of preventing mortality. It might not be unreasonable to assert that our stricter policies may have contributed to a relatively higher mortality. Yet, perhaps the biggest question here is: why are there so few questions being posed in the media in respect of the efficacy of masks, lockdowns or vaccination policies? On the rare occasion questions are raised in our national media, it as if an anti-vaxxer, right-wing loon, or political extremist is trying to gate crash what might otherwise be a rather sedate and respectable party. Pro-VaxxerIn the good old days before Covid, in Ireland, and around the world, we only vaccinated those who were vulnerable to, or at risk from a specific disease. We still vaccinate children against an array of illnesses that adults have not been, and are not routinely vaccinated against; Rotavirus and Meningitis B are but two obvious examples. Adults are equally susceptible to infection by either, but they are not as vulnerable to serious illness, and so are not vaccinated. Previously, we only ever vaccinated the vulnerable and those at risk; recently, however, that good science and common sense has been turned on its head. It is suggested that we should vaccinate young healthy people who have little if anything to fear from Covid-19. A paediatric genetic-vaccine is expected to be available later this year. It is argued that even though children are generally not susceptible to serious disease, they should be vaccinated in order to protect the vulnerable and achieve herd-immunity. In the meantime, the vulnerable have in large part already been either been vaccinated already, exposed or sadly passed away. In a recent post on Twitter Michael Levitt, Nobel Laureate and Professor of Biophysics at Stanford University said: If getting the disease does not give immunity, how do you think that a vaccine that makes the same spike protein as the virus makes will give immunity? It beggars belief that with over a quarter of a million cases of Covid-19 already confirmed in Ireland, [viii] those who have already contracted the virus, are not at least being offered antibody testing prior to being offered (or pressured into taking) a new type of vaccine; novel vaccine that have recognised associated risks, and have not completed all safety trials. Between March and June, 2020, 96% of additional deaths related to COVID-19 in Europe occurred in patients aged older than 70 years [ix] We have clearly lost sight of whom we are trying to protect, and what we are trying to protect them from. Presently we have a national obsession with conformity, and an ostensible adherence to guidelines. Despite empirical truths, and substantial contrary evidence, we are being corralled into what increasingly appears to be a specific belief-system surrounding Covid-19, and its threat to the entire population. Those who have read George Orwells Animal Farm (1945) will be familiar with the threats issued to the hapless animals: Jones the farmer will return, and destroy all of your good work! In contemporary parlance, he will return with Long Covid, [x] and frightening New Variants with him.44 Politicians have applied policies that are in keeping with this notion of universal severity in response to a virus where 86% of those infected did not have virus symptoms, such as cough, fever, and loss of taste or smell., according to a UK study from October .[xi] Many of our Covid policies arrive with the benefit of preserving established governments from demonstrations and assemblies calling for policy revisions and or enquiries. My own calls for a public enquiry into nursing home deaths, or my pleas on behalf of common sense and natural science, are at best ignored by media. As are those of colleagues who feel and believe as I do, including Limerick GP Dr. Pat Morrissey, and Wexford GP Dr Gerry Waters, who was recently suspended by the Medical Council for refusing to adhere to and promote current public health guidance. Others who have openly spoken out against current policies have been subjected to investigation by the Medical Council, and ongoing vilification by many of our peers. Speaking out returns precious few short term dividends. Throughout much of Europe since the outset of the crisis, governments, like our own, are presently controlled by proxy scientific-panels or unelected expert committees. Governments claim to be simply following their scientists advice, whilst the scientists insist that they are merely informing the government and not directing government policy. In this apparently blameless political no mans land, the stage is perfectly set for blameless political atrocities. War of the Words: Genetic vs TraditionalMany scientists and physicians prefer to describe most Covid-19 vaccines as gene therapy. It is a phrase that no doubt serves as much to antagonise proponents, as it does to inform them. However, it is as good a place as anywhere to start. Genetic vaccines are certainly not traditional vaccines. The licence for their use against Covid-19 throughout Europe was granted under emergency legislation that permits manufacturers to skip phase 4 safety trials that would have otherwise delayed their distribution. Advocates insist that skipping this final phase was absolutely necessary to resolve the current crisis. There is much to this argument, and we will not dive into it here. However, one point should be made. There are at least two off-patent (cheap and safe) drugs, Hydroxychloroquine and Ivermectin, that may be effective in treating Covid-19. These drugs are not, however, licensed for use in treating Covid in many Western countries, (particularly the wealthier ones who can afford the novel vaccines).  See article link If either, or both, drugs had been licensed, this may have proved an obstacle to the granting of emergency use licences for Covid-19 vaccines. The reason for this is that grounds for emergency licensing of genetic-vaccines are substantially reinforced, as long as there are no other pharmacological treatments available at the time. A Traditional VaccineIn China the practice of inoculation against diseases such as smallpox was established as far back as 200 BC.[xii] It is likely that traditional medicine, tribesmen and ancient civilisations used, or at least inadvertently knew something of the benefits of limited exposure to a disease, in order to establish some degree of immunity. Our own modern era of the traditional vaccine begins when Edward Jenner (1749-1823) noticed that milkmaids appeared to be relatively immune to smallpox, a viral illness that was, in Jenners day, responsible for widespread suffering and death. Jenner observed that something was being transmitted from the cows to the milkmaids, effectively protecting them against smallpox. Cows contract cowpox. Its not the same disease as smallpox, but as the respective viruses are so similar, whenever the hands of a milkmaid came into contact with a blister or pox on the udder of a cow infected with cow-pox; the milkmaid would be exposed to this very similar virus. In these instances the cowpox virus or pieces of it, would enter the milkmaids blood stream through a cut or minor abrasion on her hands. The virus would be identified by her immune system as a pathogen or disease-causing agent. White cells would attack the cowpox virus, causing it to break apart. Those same white cells would manufacture antibodies; little Y-shaped proteins that will stick to surface-proteins on the virus, and cause it to be directly destroyed, or recognised by other white cells that will mobilise to destroy it. All of this complex immunology would of course be occurring within the milkmaids blood, whilst she happily milked her cows. She might notice a slight blister, a little pus, or minor swelling around one of the abrasions on her overworked hands. The slight redness might be ignored, and would inevitably fade away. However this localised reaction would have heralded exposure to cowpox. The cowpox antibodies would then persist in her blood, remaining attached to the surface of many of her circulating white blood cells; protecting her or vaccinating her against small-pox. If the milkmaid should later come into contact with smallpox, those newly formed cowpox antibodies would be ready to mount an early and more efficient immune response. Her antibodies to the cowpox virus could attach to the smallpox virus, recruit other white cells killer t-cells etc onto the scene, and mount a pre-emptive response. This would be fast enough to eradicate the smallpox infection before it had an opportunity to spread and cause severe illness or death. It was Jenners genius that ultimately brought this reality to light. Jenner collected some of the pus that oozed from the udders of cows infected with cowpox. He swirled it about in a drop of water, placed it in a glass vial and then offered it to the world as the prevention for small-pox. Half a century later Louis Pasteur coined the phrase vaccination after vacca, the Latin for cow. The paradigm in respect of human medicine and public health had shifted forever. Perhaps the real hero of the vaccination story was an eight-year-old boy by the name of James Phipps, the son of Jenners gardener. On May 14th 1796, Jenner made a small incision into Jamess arm, and rubbed in a drop of his magical pus-paste, making little James the first to be given a vaccine in the modern sense. Thankfully, little James proved immune to the various small-pox exposures and challenges that Jenner then came up with. At the time, small-pox was responsible for almost 10% of annual deaths in England. Jenner sent his results in a paper to the Royal Society for publication, but he was dismissed as an eccentric and his paper was ignored. Having had the audacity to suggest pus from an infected cows udder, as a cure for smallpox, Jenner was at first dismissed by his peers as something of a quack. Yet, rather than disappearing into obscurity, he persisted. He vaccinated a further twenty-three people, and having seen little James survive, he even included his own eleven-month old son Robert, in this first ever vaccine trial. At that stage the medical establishment found it impossible to ignore his findings, which soon attracted widespread interest amongst the medical fraternity. However, it was not until 1840, some forty-four-years after his first attempt to publish his results, that the British Government began offering Jenners vaccination, free of charge, to the general public. The same but differentSince Jenners day, traditional vaccines have functioned in precisely the same way. Pharmaceutical companies take a virus or bacterium, they break it up, kill it, or leave it intact but render it weaker or ineffective the same but different. They then take the bug (or pieces of the bug), swish them around in a little drop of water, add in a few elements that act as preservatives and immune-stimulants; then we doctors inject those pieces into people, thereby preventing many from succumbing to various infective diseases. The vaccination exposes us to a bug or pieces of a bug causing our immune system to generate antibodies and white blood cells that will persist in our circulation and be ready to launch a pre-emptive strike against the bug or a similar bug if it is encountered again: we have, in essence, become immune. So what is different about genetic-vaccines? Well heres where the story becomes a little nuanced. Lets try to put it in terms we might relate to. To begin with we must remind ourselves that: all living things are composed of cells, which is perhaps the most basic tenet of biology. Viruses are not considered living things, because they are not cells and neither are they made up of cells. They are formally referred to as obligate intracellular parasites. They only become alive; and can only replicate, after entering host cells, at which point they replicate or multiply within host cells. Once inside a cell the virus hijacks the cells own processes for making things that the cell needs for itself. The infected cell then becomes a virus factory, it swells with new virus particles, until it bursts, dies, and releases its payload of new virions into the bloodstream, or fluid outside of the cell membrane. It is only when a virus is outside the cell, within the blood stream or tissues, that it might be recognised by white cells or antibodies, and become the subject of an immune response. When a virus is inside one of our cells, there are some discrete ways this cell can let other cells know that it has become infected; there are means by which the immune system detects that one of our own cells has a virus inside it. However, these are comparatively slow, indefinite and uncertain processes and will not be discussed here. The major and most important way the immune system clears viruses is by getting at them before they get inside our cells. Once a virus is inside a cell, for the most part, it is hidden from the immune system. This point will be crucial to understanding the distinction between a genetic vaccine, and a traditional vaccine. 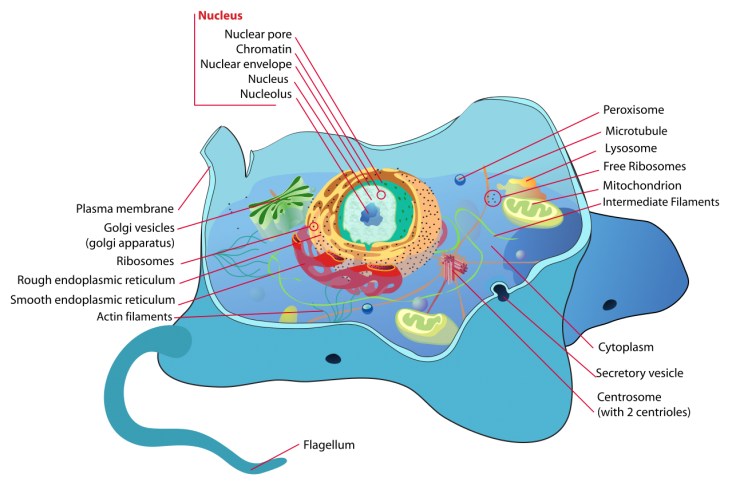 All Cells Look a Little, or a Lot, Like a Fried Egg:Under a microscope, all cells appear a little like fried eggs. Almost all of them have the same basic plan, the yellow yolk being the nucleus; the white of the egg, the cytoplasm; and the outer margin of the fried egg (the crispy brown edge) being the cell membrane or wall surrounding the cell. To learn the basics of how genetic vaccines work, we need only refer to this analogy, but we must understand our egg a little better before we put the toast on. The yellow yolk, or nucleus, contains all of our DNA. To understand what DNA looks like, imagine your fly, not the one buzzing at the window, but the zip on your trousers. It is composed of two sides or strands that are linked together when your zipper is up, and separated when your zipper is down. DNA is like an extremely long length of closed zip. Imagine this super long zip coiled into individual space-saving packages, like neat balls of wool. Each of these little packages is called a chromosome and (with the exception of sperm cells and egg cells) the nucleus of each of our cells contains forty-six of these little balls of wool; twenty-three from mum, and twenty-three from dad. All forty-six are packed into the nucleus, the yellow yolk of our analogous egg. When we, or one of our cells, needs something; a protein, a hormone, a replacement part etc., the information to make what the cell needs (the recipe for all of lifes necessities) is coded for in that length of closed zip, our DNA. Each of the teeth along the length of the zip strands, represent a single letter of the genetic code. An entire message may contain many letters, or teeth, along a specific length or piece of the zip. The lengths of zip that contain messages (or recipes) are called our genes. The message within a gene is like a recipe in a cookbook. It contains a coded instruction for how to make the protein, enzyme etc., or whatever it is that the cell wants or needs. The DNA code is in the nucleus, and the basic ingredients are located in the cytoplasm, and it is in the cytoplasm (the egg-white) where the item required is assembled and manufactured. The raw materials for manufacture get into the cytoplasm, when they are absorbed across the cell membrane (the crispy brown bit at the edge of our fried egg). These raw materials are the amino-acids, sugars and vitamins etc., that we receive in our diet. To kick off the process, when a cell needs to make something, a signal is sent from the white of the egg (the cytoplasm) into the nucleus. That signal makes its way to the ball of wool or chromosome that contains the particular recipe, or code for the ingredients that will make up whatever is needed by the cell. When the signal reaches the chromosome containing the particular recipe or gene, the ball of wool is loosened slightly, and a relatively small length of closed zip (or DNA containing that recipe), is unzipped. One side of the opened zip is then copied into a piece of mRNA. That copy of one side of the unzipped zip is called messenger RNA. In most textbooks it (the mRNA) looks exactly as I have described it: a single side of a zip. This messenger RNA then exits through pores in the nucleus. It enters the white of the egg, where this mRNA recipe is then read or translated, and whatever it is the cell needs can now be manufactured within the cytoplasm or the white of the egg. The RibosomeWhen the strand of messenger RNA leaves the nucleus and enters the cytoplasm it is immediately found by a fascinating little cytoplasmic protein called a ribosome. The ribosome attaches to the mRNA. It then slides along this single strand of zip, and as it does so, reads the code, and then makes a little strand, like a bead of pearls (a polypeptide). That strand of polypeptide then curls and folds itself into a little ball or blob; and this little blob of protein, is the very thing that the cell was looking for in the first place. It might be a structural protein, an enzyme, a building block, a replacement part, or whatever. When the ribosome slides along the piece of mRNA it makes this new little string that will ultimately fold upon itself to become the required product. This wonderful orchestral process is as ancient as life itself and is called translation. It is one of the rare occasions when jargon makes sense, for the little piece of mRNA, has indeed been translated into a protein or final product by the ribosome. The cell has now manufactured the thing that it needs, and after a few translations, the mRNA then degrades. No more ribosomes can attach to it, and no further product can be manufactured from it. If the cell wants another product it must send another message into the nucleus and call for another mRNA copy to be made in the nucleus and sent into the cytoplasm. It is a beautifully organised process, integral not simply to human life but to all life on the planet. How Does a Genetic-Vaccine Work?If you got all of that, you have grasped some of the fundamentals of cell biology and we are now able to ask: how does a genetic vaccine work? Most of us have seen an image or an artists impression of what a coronavirus looks like. A little ball, covered in spikes, like a medieval weapon swung from the end of a chain. Inside this little ball are the viruss own genes. These genes are in the form of strands of RNA; the same type of RNA that is made in the nucleus of our cells, and sent into the cytoplasm for the manufacture of all things that the cell needs. The main difference between the RNA strands within a coronavirus, and those that naturally emerge from the nucleus of our own cells, is that coronavirus RNA does not code for things that our cells might need. On the contrary, it codes for pieces that make up the coronavirus itself. When a coronavirus binds to the outside of one of the cells in our respiratory tract, it releases its RNA into those cells into the white of the egg and there, instead of making proteins that are needed by our cells, our ribosomes attach to their viral RNA and begin to manufacture (or translate) proteins that make up the physical structure of the virus. The host cell has now becomes a virus-making factory; the cytoplasm swells with viral particles; the cell bursts, and thousands of new viruses (virions) are released into the bloodstream, or the fluid that lies outside of the cell membrane. A genetic vaccine looks like, and functions, in almost exactly the same manner as the coronavirus itself. If a genetic vaccine could be visualised, it would look like a little sphere that encapsulates a piece of viral RNA or DNA (depending on which of the four vaccines we are considering). The role of the sphere is to protect the RNA or DNA inside the vaccine, and, most importantly, to bind it to human cells in a manner that will allow the piece of RNA or DNA to enter host cells at the site where the vaccine is injected. For an RNA containing vaccine (Pfizer & Moderna) once the vaccine RNA gets inside our cells, our ribosomes attach and translate the RNA into a piece of the virus (one of the spike proteins). The host cell will then swell with spike proteins, and release them into the blood stream or body fluids outside the cell. There, the spike-protein will trigger the same immune response that Jenner and the traditional vaccines make use of. For DNA vaccines (Johnson & Johnson, AstraZeneca) the vaccine-DNA makes its way into the nucleus of our cells where it begins working (and is treated the same as our own DNA). It is copied into a piece of mRNA that will then travel into the cytoplasm and be translated by ribosomes into spike-proteins. Because genetic vaccines cannot infect cells, the process whereby a genetic-vaccine enters host cells is referred to as transfection. It is only after the transfected host cell releases spike-protein into the blood stream that our genetic-vaccine begins working in the traditional way. In reality, it is the cellular process for the manufacture of things which has been hijacked, and the traditional vaccine is being made inside ones own cells. The vaccine is released into our blood stream in the same way that a cell infected with a virus releases new virus into the blood stream or tissues. The final result might be the same, however, where a genetic-vaccine is different is in its mechanism it operates inside cells at a level of intimacy that Jenner could never have imagined. Because DNA vaccines enter the nucleus of our cells, and are treated as our own DNA, they come with a risk of damaging our own DNA, causing mutations, including, potentially, cancer. The potential is indeed an established fact. It is no less established than the fact that there is a link between smoking and cancer. Consider when a piece of synthetic DNA comes within intimate proximity of a relatively enormous coiled ball of DNA that is dynamically unwinding and unravelling in response to the daily activities of the cell. Is there a chance that this relatively small piece of synthetic DNA might become incorporated into or interfere with the normal function of our own DNA? Before Covid, the answer was an emphatic yes. However of late, the mere suggestion will undoubtedly be treated as something of a conspiracy theory. It is for this and other reasons that genetic-vaccines have not been previously licensed for use in humans prior to the current crisis. Thus, a 2013 paper[xiii] published in Germs, the respected Journal of Infectious Diseases lists the established disadvantages of DNA vaccines. Crossing the RubiconAt this point the reason critics refer to current Covid-19 vaccines as gene therapy should not be too difficult to understand. It is important to bear in mind that as the cellular process of translation can be hijacked to produce a vaccine, it can also be hijacked to produce a myriad of other potential pharmaceutical therapies. Very limited forms of gene therapy are available in the treatment of terminal cancers. However, pharmaceutical companies have not been able to market this form of medicine, outside of the laboratory, on human populations.[xiv] A cynic might reasonably argue that companies are exploiting the current crisis in order to expedite safety trials and open the market for gene-therapy. There is nothing new here, this type of therapy, whereby patients are administered the gene for a missing or desired product, has been in development for several decades. The major difficulty for pharmaceutical companies has been how to get it out of the laboratory and past the paralysis of safety trials. It is certainly easy to see that if our cells are programmed to make and release spike-proteins, they can also be programmed to release other kinds of proteins, drugs and potential therapies directly into the human blood stream or tissues.[xv] Getting this type of therapy past regulators, and avoiding meaningful debate, has, (for better or worse), clearly been accomplished within the context of the current crisis. From a simple economic perspective, if human cells can be programmed to take on the role of manufacturing the drug, numerous difficulties in respect of production, costs, delivery, and even safety trials, are relatively easily overcome. The paradigm shift that resulted from Jenners development of vaccination could pale into insignificance compared to the potential game changer of genetic-vaccine. Ah go on. Youll be grand!If, indeed, these vaccines are going to protect people from Covid-19, and they come with the added benefit of paving the way for novel therapies, why are people like me getting our proverbial knickers in a twist? Again the answer is not that complicated. The cellular process of translation that is being hijacked by the relevant pharmaceutical companies, does not belong to them, to our respiratory cells, or even human cells. As mentioned already, it is a process that belongs to ALL cells, in ALL species. In essence it belongs to all living things in Nature. If anything happens to go wrong, the consequences are not limited to human beings, as the process being hijacked is not exclusive to us. It belongs to all life on Earth. The consequence of error, may extend further than a little nausea or swelling at the injection site.[xvi] Potential consequences extend to all cells that utilize the same process, and come in contact with the manufactured DNA or RNA. DNA or RNA? Red or White?Whilst the potential for either of the two available DNA vaccines to integrate into, or damage, human DNA is well established; there is an argument being made that this cannot possibly occur with the two available RNA vaccines. Generally speaking within our cells once RNA is copied or made in the nucleus it moves into the cytoplasm. It does not travel backwards. RNA does not move back inside the nucleus and incorporate into our DNA. However, the key words here are: generally speaking. Nature (generally speaking) blocks this possibility because the copied RNA that exits the nucleus, is different to DNA. It is an RNA copy of the DNA, the RNA cannot bind or interact with DNA. In the first instance RNA is a single stranded copy of one side of the zip. In the second instance the teeth on the newly copied RNA are slightly different. They are tweaked with a sugar molecule called ribose, they are ribosylated and therefore cannot readily recombine with DNA. (The R in RNA simply means Ribosylated Nucleic Acid.) The RNA does indeed code for the same message that is contained within the DNA, but the teeth, or the letters of the RNA code, are slightly different. RNA does not travel backwards and interfere with DNA. Generally speaking they are incompatible, and cannot interfere with each other. Therefore, when the vaccine makers insist that the pieces of RNA that they have transfected into our cells do not interact with our DNA; well, they arent spoofing. It doesnt normally happen that RNA interferes with DNA. So thats what it says on the tin. However, there are two points that must be considered before we take this claim at face value. The first is a question of precedence and the second is a question of scale. Does it happen in humans and in Nature that RNA can travel backwards into the nucleus and interfere with or incorporate into DNA? The simple answer to this question is a definite yes! RNA can and does travel backwards to incorporate itself into our DNA. This retrograde move, (where RNA sequences become incorporated into DNA) is called reverse-transcription. The reason for the use of retro in the word retrovirus, is because retroviruses, and many other viruses, make use of reverse-transcription, converting RNA into DNA that will then integrate into our own DNA HIV and HTLV (a human virus that causes t-cell leukaemia) are examples of viral infections, where RNA is converted backwards into DNA which then interferes with our own DNA inside the nucleus of our cells. These viruses contain RNA, and they also carry an enzyme called reverse transcriptase. This enzyme converts RNA backwards into DNA. Retroviruses and other viruses (such as Hepatitis B) introduce the reverse-transcriptase enzyme into our cells when they infect them.[xvii] Furthermore, our own cells normally produce and use this enzyme (reverse transcriptase) inside the nucleus, where it has some house-keeping roles in maintaining our own DNA.[xviii] Perhaps even more interesting is the fact that within the human genome some 8% of our DNA is composed of DNA that was originally viral RNA. Infections with RNA viruses whose genes have since become permanently incorporated into our own DNA. These sequences are called Human Endogenous Retroviral Sequences or HERVS.[xix] Many of them persist within our genome because they may code for proteins or things that are likely to be of some benefit to us; genes brought into our genome from outside the cell, via the natural, dynamic interaction between viruses, retroviruses and human DNA. Many more of these endogenous retroviral (originally RNA) sequences are mysteriously redundant, and science is yet to learn of their function in sickness or in health. The fact remains that they are present; been present for countless millennia; may be integral to our evolution as a species; and are certainly with us until death do us part. They should serve to remind us that there is a long established history of communication between viral and human genetics; an interaction that we should attempt to understand before it is blindly manipulated. InterconnectednessToo often viruses are portrayed as static structures, distinct from our own genetic material and distinct from one another. This is quite simply a rather primitive concept, the same kind of thinking that removes human beings and the consequence of our actions from Nature. It is part of the reason we remain largely incapable of seeing and appreciating the vast web of interconnectedness that dependently joins us to whales, rain forests, and even viruses. We depend upon viruses for our genetics, as we depend upon yeast for our beer. Often viruses depend upon each other to cause infection. In certain instances, if a particular virus is missing something, a part or component (without which it is defective or deficient), the missing part is supplied by another helper-virus. There are helper-viruses, and there is an entire family of viruses (dependoviruses) that are entirely dependent upon assistance from helper-viruses. For example, in Humans, Hepatitis D virus is activated, only in the presence of Hepatitis B virus. Essentially, in order to function, the D-virus borrows some missing parts from the B virus. In short, viruses are not monogamous recluses: interacting with each other; helping each other; interacting with our genetic material within the cytoplasm and within the nucleus. It does not matters if that genetic material has come from the nucleus of our own cells, or been synthesized in the labs at Johnson and Johnson.[xx] A Question of ScaleThere is no such thing as a perfect process. Do something for the first time and you might do it right, do it right enough times, and you will eventually do it wrong. When vaccine RNA or DNA hijacks a natural cellular processes and transforms the cell to vaccine or spike-protein production; how many times does this event occur in the tissue of the person who has thus been vaccinated? Thousands, or several thousands of times? How many times has it occurred when several billion people are vaccinated? I dont know the answer to this question. However, when a process is repeated billions of times, mistakes are no longer possible, they are inevitable. Such mistakes or mutations are not only inevitable but are essential, lying at the heart of evolution itself. The End is Nigh?There is certainly a mountain of spin and delusion on either side of the genetic-vaccine or gene-therapy debate, and we must keep matters in perspective. Genetic modification is here to stay, for better or for worse. The argument in respect of unforeseen genetic consequence to ourselves and/or other species is an old one. It began with Dolly the sheep, and has raged for some time around the desirability of genetically modified foods. Ironically, the introduction of synthetic genes into vegetables, created something of an international furore, yet the transfection of synthetic genes into millions of regular human beings has created far less controversy. Debate or discussion on the subject of genetic modification or therapy, its necessity, utility, or potential harm, is long overdue; although perhaps it might be a case of too little, too late. Today, many of the foods we eat have been genetically modified to some degree. Genetically modified food is, however, met with and processed by the acid and digestive enzymes in our guts. The synthetic genes in GM products do not (as far as we know) enter our cells, they do not attempt to manipulate our own cellular or genetic processes. There is clearly an urgent need to revisit this debate in light of these new vaccines. The battle may have been lost in respect of GM crops, but there is a reasonable argument to be advanced this time round as human genetic processes are being tampered with, rather than sheep, beetroot or soya beans. The Right Hashtag?In recent years discourse and protest have become strangely predictable, organised around or stimulated by whatever happens to be trending on social media. It seems the right hashtag hasnt been developed for debate in respect of current pandemic policy, even as that policy extends into the function of our own cells. How many people in Ireland, or around the world, know how a Covid vaccine works? How many clinicians are aware for that matter? When debate does erupt in relatively small pockets around the country it is hijacked by extremists or dismissed as being organised and attended by extremists. Social media appears to be moderating our behaviour to a greater degree than even genetics. The health of our society depends far more on constructing a more honest and happier version of ourselves. We need to re-evaluate materialism, define happiness, reduce consumption, eat less (or no) meat, take plastics out of our food chain and ecosystems, restore and preserve habitats, protect and understand a biodiversity upon which we are entirely dependent. All of this, and more, is not contingent on genetic modification, no more than it is dependent on us getting to Mars. Therefore, for the reasons I have outlined, I would not inject a healthy animal with an experimental genetic-vaccine, never mind a healthy human being. [i] Jonathan Corum and Carl Zimmer, How the Oxford-AstraZeneca Vaccine Works, New York Times, March 22nd, 2020, https://www.nytimes.com/interactive/2020/health/oxford-astrazeneca-covid-19-vaccine.html [ii] Smriti Mallapaty, The coronavirus is most deadly if you are older and male new data reveal the risks August 28th, 2020, https://www.nature.com/articles/d41586-020-02483-2 [iii] Adam W. Gaffney, We need to start thinking more critically and speaking more cautiously about long Covid Statnews, March 22nd, 2021, https://www.statnews.com/2021/03/22/we-need-to-start-thinking-more-critically-speaking-cautiously-long-covid/ [iv] Conor Pope, Vivienne Clarke, Vaccination rollout in nursing homes almost complete, HSE says, February 12th, 2020, Irish Times, https://www.irishtimes.com/news/health/vaccination-rollout-in-nursing-homes-almost-complete-hse-says-1.4483250 [v] CSO. https://www.cso.ie/en/releasesandpublications/ep/p-covid19/covid- 19informationhub/health/covid-19deathsandcasesstatistics/ [vi] Moderna Announces First Participants Dosed in Phase 2/3 Study of COVID-19 Vaccine Candidate in Pediatric Population https://investors.modernatx.com/news-releases/news-release-details/moderna-announces-first-participants-dosed-phase-23-study-0 [vii] CSO. https://www.cso.ie/en/releasesandpublications/ep/p-covid19/covid- 19informationhub/health/covid-19deathsandcasesstatistics/ [viii] https://www.google.com/search?client=firefox-b-d&q=covid+deaths+ireland [ix] Immune evasion means we need a new COVID-19 social contract, The Lancet, February 18th, 2021, https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(21)00036-0/fulltext [x] Jeremy Divine, The Dubious Origins of Long Covid, Wall Street Journal, March 22nd, 2021, https://www.wsj.com/articles/the-dubious-origins-of-long-covid-11616452583 [xi] Angela Betsaida B. Laguipo, 86 percent of the UKs COVID-19 patients have no symptoms, News Medical Life Sciences, October 9th, 2020, https://www.news-medical.net/news/20201009/86-percent-of-the-UKs-COVID-19-patients-have-no-symptoms.aspx [xii] The History of Vaccines, Chinese Smallpox Inoculation, https://www.historyofvaccines.org/content/early-chinese-inoculation [xiii] Germs. 2013 Mar; 3(1): 2635. Published online 2013 Mar 1. doi: 10.11599/germs.2013.1034/ [xiv] Kristina Fiore, Want to Know More About mRNA Before Your COVID Jab? Medpage Today, December 3rd, 2020, https://www.medpagetoday.com/infectiousdisease/covid19/89998 [xv] Nature Reviews Drug Discovery volume 17, pages261279(2018) [xvi] Nicola Davis, Covid vaccine side-effects: what are they, who gets them and why? The Guardian, March 18th, 2021, https://www.theguardian.com/world/2021/mar/18/covid-vaccine-side-effects-what-are-they-who-gets-them-and-why [xvii] Medical Microbiology. 4th edition (Chapter 62).Galveston (TX): University of Texas Medical Branch at Galveston; 1996. [xviii] Proc Natl Acad Sci U S A. 1986 Apr; 83(8): 25312535. doi: 10.1073/pnas.83.8.2531, https://www.nature.com/articles/1205081 [xix] PMCID: PMC7139688 PMID: 32155827 Human Endogenous Retroviruses (HERVs): Shaping the Innate Immune Response in Cancers. [xx] Knipe, David M.; Howley, Peter M. (2007). Fields Virology (5th ed.). Lippincott Williams & Wilkins. pp. 1267. See also: Covid-19 in Ireland: Landfall at https://cassandravoices.com/science-environment/science/covid-19-in-ireland-landfall/ Add Your Comments >>  printable version with comments printable version with comments   |

















 Digg this
Digg this del.icio.us
del.icio.us Furl
Furl Reddit
Reddit Technorati
Technorati Facebook
Facebook Gab
Gab Twitter
Twitter
|